When I was in college, I applied for an internship at the Huffington Post, that venerable bastion of journalism. Before my interview, I was given a spreadsheet of articles and associated view counts. I was asked to formulate and present a hypothesis about which types of articles generate the most views.
When I presented my hypothesis, I intended to present it like a science paper: introduction, methods, results. But, 5 minutes into my presentation, my interviewer, Koda, stopped me.
“Always start with the most exciting result first,” he said. So, I restarted my presentation, skipped to the end of the slides, and worked backwards.
I didn’t end up getting the internship. But, in honor of his advice, here’s the most exciting figure I’ve ever seen in a dementia paper. I’ll start from this figure, and work my way backwards.
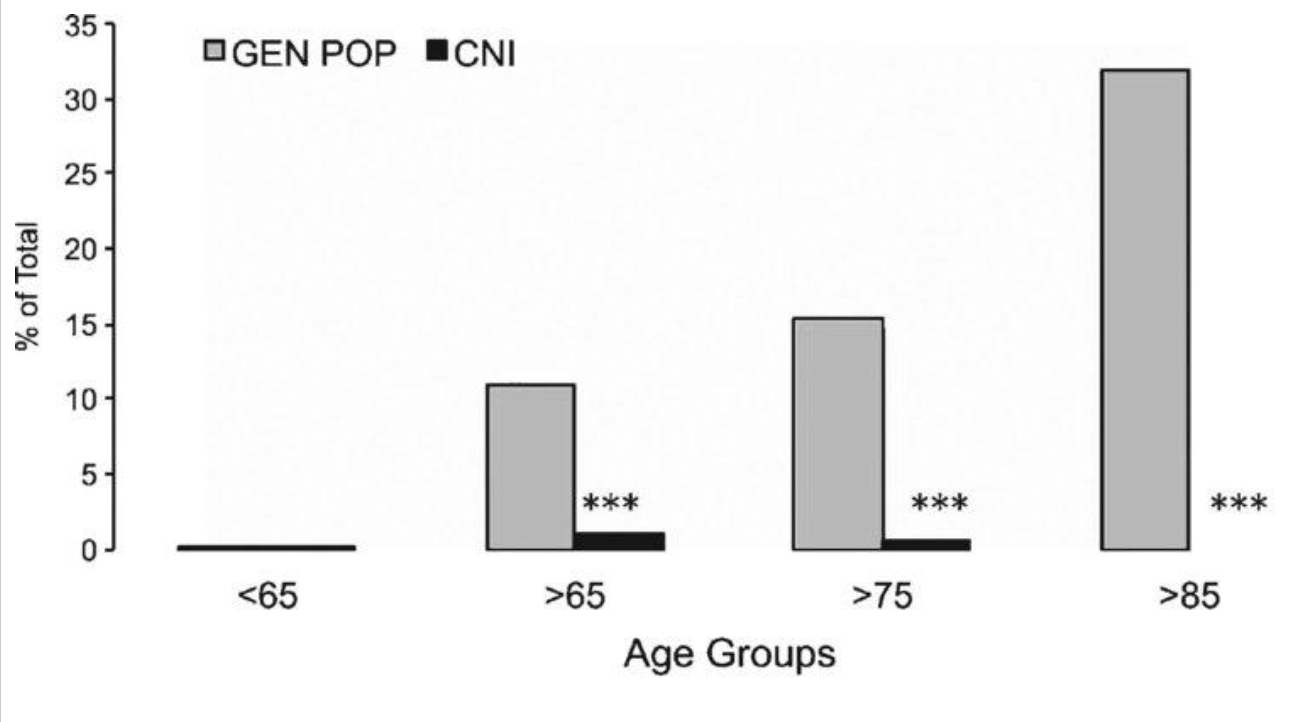
This is a graph of dementia rates in immunosuppressed organ transplant patients at a University of Texas hospital. Specifically, these are organ transplant patients who have received calcineurin inhibitors, which is a specific type of immunosuppressant with some weird properties.
The gray is the percentage of patients in the general population in that age group who get dementia. The black is the percentage of organ transplant patients in that age group that have received calcineurin inhibitors who get dementia.
As you can see, dementia is almost absent in the calcineurin inhibitor group. It is literally absent in the >85 group. Shocking, no?
And before you think this is just some trick with percentages, here are the raw numbers below.
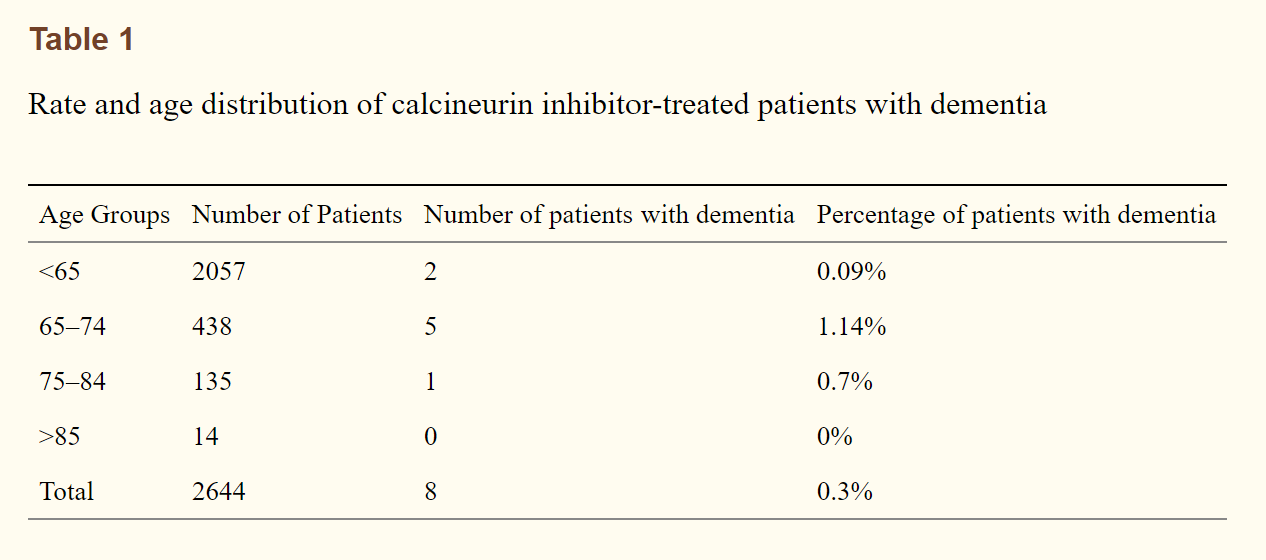
We’re not talking about small numbers of people here. These are large groups of people, and dementia is almost completely absent. Like…holy shit, no? If you take this graph at face value, it kind of looks like calcineurin inhibitors are a preventative or a cure for dementia. Given that Biogen’s bullshit drug for Alzheimer’s was estimated to bring in so much revenue as to bankrupt Medicare, this is a $50 billion discovery at least. Maybe a Nobel Prize, too.
But, before we pop the champagne, let’s take a step back and see if we can actually soberly address this. I’ll start with a small confession, then I’ll discuss why you might not believe this paper, why you might believe it, and then what we should do about it.
So, first of all, the confession: I’m not a neutral observer here. In talking about this paper, I’m talking my own book. My company, Highway Pharmaceuticals, is currently raising funds to get a safer, easier to use, extended-release version of cyclosporine, the most common calcineurin inhibitor, into first-in-human trials. If this paper is correct, investors should probably consider throwing money at me.
Now with that out of the way, there are some major reasons why you might not believe this paper.
The most obvious reason that most people think about is survivorship bias. Organ transplant patients are, by their nature, sick patients. Maybe immunosuppressed people who would get dementia are also the sort who would die sooner, possibly because they forget to take their meds and then their body rejects the graft.
This is possible, but seems unlikely to me, as you wouldn’t expect there to be a strong enough correlation to account for the huge disparity in dementia results. This paper (which I discuss much more below) suggests organ transplant patients with dementia are about twice as likely to experience graft loss, although it’s unclear which way the causative relationship swings. Side note: I also found a hilarious, weird study that stated “a greater fear of repulsive animals” is associated with graft rejection. That has nothing to do with anything, but I thought it was funny.
You might also wonder if it has to do with the diet and exercise routine that transplant patients are encouraged to adhere to after transplants. After all, diet and exercise are protective against dementia.
Well, in the words of the original study author, compliance with diet and exercise regimes is “limited”, and wouldn’t explain these results. Besides, people who get organ transplants are unhealthy people to start with and have very high rates of diabetes and obesity (major risk factors for dementia), so diet and exercise regimes are unlikely to totally reverse this.
The last reason you might think this isn’t real is to me the most persuasive: it hasn’t been replicated. The paper from above that examined dementia and graft loss risk was looking at national Medicare data for kidney transplant recipients in general, and it also found that the 10 year risk of dementia in these patients was much more similar to the general population: 12% for ages 65-70, and around 20% for 75+. It also, surprisingly, found that people who weren’t on calcineurin inhibitors had a smaller risk of dementia, the exact opposite of the original paper.
This is the hardest to explain, as these numbers clearly contradict the University of Texas numbers. It can’t be a difference of organ transplants vs. kidney transplants, either, as the University of Texas organ transplant population is majority kidney transplants.
There are only a few possibilities to explain this, in my mind:
1. Randomly, very few patients who would eventually get dementia ended up in this Texas hospital receiving organ transplants. This would be strange, as Texas in general does not have different dementia rates than the rest of the country.
2. Someone messed up their data. This would be a pretty huge mess up on someone’s part, but it could be something as simple as how dementia is reported.
For the University of Texas study, they got their dementia reports from physicians’ notes, presumably in their electronic medical records. For the Medicare data, they got their dementia reports from the Medicare claims. This study gives a sensitivity and specificity of Medicare claims for dementia at around 85% vs. doctors’ diagnoses, which seems pretty good, but that’s looking at only 700 records from 1993-2005 vs. 40,000 records from 1999-2011 in the Medicare dementia study.
I can’t know a priori which study is more likely to mess up their data. However, what we can say is that the dog isn’t barking: calcineurin inhibitors are used a lot for organ transplants, and nobody else is reporting an effect on dementia.
Someone else should have noticed, especially because the UTexas paper was published in 2015. It’s easy for me to believe that hospitals in general do not see an absence of dementia in organ transplant patients, but I don’t have an opinion on whether the UTexas patient population is actually absent of dementia.
3. There’s something different about how the University of Texas hospital administers calcineurin inhibitors vs. the average hospital.
This is entirely possible. Calcineurin inhibitors are dangerous and difficult to administer correctly, so it’s possible one hospital has developed a unique protocol. This unique University of Texas protocol might be the difference between these two studies.
Overall, though, I’d say this is a definite reason to be cautious about the University of Texas study. Obviously, I’d like the data to be true, but I understand if people have their doubts. For my own part, I’ve contacted authors of both papers, but haven’t received substantive responses from either. I’ll update this post when/if I do.
But, instead of ending on that, I want to discuss, instead, a scientific reason why I think calcineurin inhibitors might actually work in dementia, and why my personal balance tips more in favor of the University of Texas study being real: the mitochondrial dysfunction hypothesis for Alzheimer’s.
The mitochondrial dysfunction hypothesis for Alzheimer’s is straightforward enough. Mitochondria, as we all know, are the powerhouses of the cell. They are little, self-contained organelles that generate ATP, the fuel for the cell.
Mitochondria are really complex. They act somewhat like their own little organisms themselves, and, in fact, that’s probably what they originally were. They have an intricate structure; their own, separate genome from the rest of the cell; and engage in constant signalling with the rest of the cell, most notably by calcium (Ca 2+) signalling.
They are also very involved in cell death, or apoptosis. This makes sense: if you’re a cell, and your powerhouse goes out, you’re probably not long for this world. This apoptosis can be planned (i.e. if the cell is infected or cancerous) or unplanned (i.e. if something damages the cell or mitochondria).
One of the ways in which mitochondria can apoptose is by the opening of the mitochondrial permeability transition pore (MPTP). This MPTP is exactly what it sounds like: it’s a pore, or opening, on the inner membrane of the mitochondria. The inner membrane is the part of the mitochondria that contains, basically, the parts of the mitochondria that generate ATP.
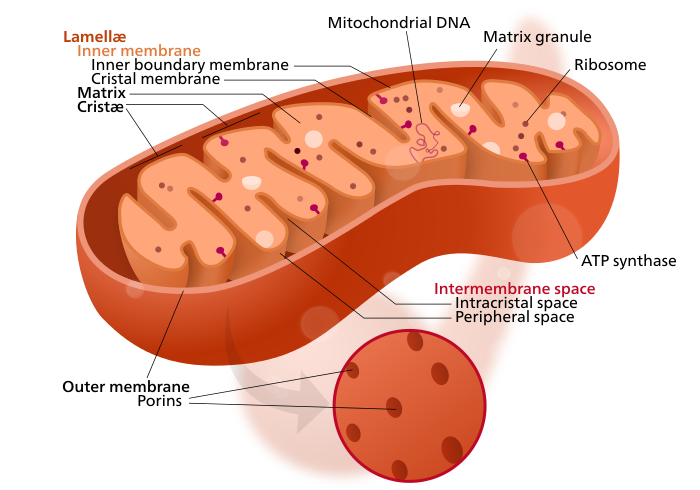
Generating ATP is a complex, chemical process that requires precise control of which ions end up where. Opening up a pore into the inner membrane of the mitochondria is somewhat similar to flinging open the door to a hermetically sealed laboratory or having a bunch of people walk on stage during a dance recital. It messes things up pretty completely.
Now, you may ask why such a door exists, considering that opening it for long enough kills the mitochondria, and opening it for a little bit doesn’t seem to do much good. The answer is… we don’t know. It might have a purpose in the body now, or it might be a holdover from when mitochondria were separate organisms. One of the things we do know, however, is how to open it. Cell stress, Ca 2+ signalling, and physical trauma to the cell all do the trick.
We also know how to keep the door closed, and that’s where we come back to calcineurin inhibitors. One of the main calcineurin inhibitors is cyclosporine. One of the main proteins that opens the MPTP is cyclophilin D, named so because it loves (philo) cyclosporine. Cyclosporine freezes the protein in place, preventing the MPTP from opening.
So, that’s how cyclosporine could work in saving the mitochondria in Alzheimer’s disease: by preventing the MPTP from opening during times of cell stress or trauma. What’s our evidence that it actually does work that way?
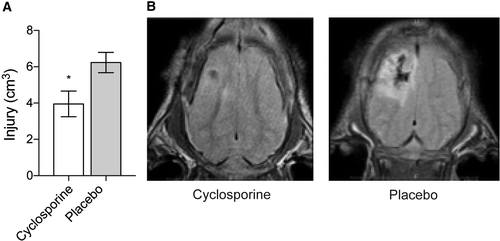
Well, first, there’s good evidence that cyclosporine can save some neurons from death when they experience stress. Specifically, when they bonk piglets on the head really hard, the ones that have been receiving IV cyclosporine for the last 5 days have a smaller hole in their brain.
Second, there’s ok evidence patients with Alzheimer’s have altered mitochondrial function. Alzheimer’s brains use less glucose, less oxygen, and have reduced enzymatic activity related to glucose. Scientists that have used mitochondria from Alzheimer’s brains in new cells have found that the new cells have reduced enzymatic activity as well, suggesting the reduced enzymatic activity comes from the mitochondria.
So, all together, if we think of the damage to the brain that results in dementia as somewhat similar to the damage to the brain from a bonk on the head, then we can believe that cyclosporine could be beneficial for preventing or treating dementia.
So…what next? Well, as I mentioned, I’m trying to raise funds to actually test this. The methods still need to be worked out, as giving a bunch of old people cyclosporine for 20 years to see if they develop Alzheimer’s is nobody’s idea of a good study to run.
However, using alternative biomarkers for a shorter period of time could be much more feasible. This is especially true if we’re looking at a vulnerable population who’s more likely to develop dementia sooner, like people with Parkinson’s, as they already have a validated biomarker for dementia: brain-glucose metabolism.
If this sounds interesting to you or you think you could help me with this, let me know. Otherwise, feel free to tell me why you think this is silly. Happy to hear feedback either way.