Table of Contents
- Introduction
- How can you be sure you have IBS?
- Steps to treat IBS
- Evidence
- Helpful info from Wikipedia that I didn’t feel like checking
Note: I’ve expanded this blog post into a full-length book! Check it out!
Introduction
I went through my own bout with IBS some years ago. It was really frustrating. It seemed to come out of nowhere. I spent a lot of money on a test for SIBO to see if that was the problem, but didn’t see any results. Then, it briefly seemed like I was cured, only to randomly become sensitive to gluten for a year.
Dealing with IBS was especially frustrating because of the unhelpful advice from doctors, family, and friends. Doctors would tell me it was all in my head. My family thought I had Crohn’s. My friends just would get weirded out by the things I refused to eat, and try to nag me into trying just one muffin/beer/hot wing.
A few years ago, my IBS disappeared as suddenly as it came. Now, I’m mostly ok. But I still remember how frustrating and life-impairing IBS was.
This article is what I wish I had back when I first got IBS. It’s not just another blog spam on the front page of Google, with the 5 things that literally every other blog spam tells you about IBS.
It’s a comprehensive guide to making sure you have IBS and not another disease, and then treating IBS. And I mean comprehensive. If I missed anything, tell me!
At the end of the article, I list all my sources (and there are a lot!) and what I took from them. I also include my evaluation of the treatment options, as I know that can be an especially challenging thing for IBS patients to do.
If you’re pressed for time, just scroll down and look at the tables. If you’re not, feel free to read everything.
How can you be sure you have IBS?
IBS is a diagnosis of exclusion. If you don’t have other conditions that can also cause stomach problems, then you probably have IBS.
Most doctors skip straight to diagnosing IBS without thoroughly checking whether you might have these other conditions. That’s unfortunate, because, unlike IBS, some of these other conditions actually have cures. If you’re diagnosed correctly, your IBS could be solved a lot quicker.
Also, some of these conditions are much more serious than IBS. So, you definitely want to make sure you don’t have these other conditions, because, if you do, you’ll need to start treating them ASAP.
Here’s a pretty exhaustive list of conditions that mimic IBS. Each row is a separate condition. Use it to potentially diagnose yourself. You’ll need laboratory tests to confirm whether you’re correct, but at least you’ll be able to advocate for yourself at the doctor’s office.
Note that the more of these conditions that you have, the more likely the diagnosis is. So, if you take the first example, an obese smoker on prednisone with constipation is more likely to have diverticulitis than a skinny non-smoker with diarrhea.
Also, please note that I’ve italicized the most important parts of a diagnosis. For example, unexplained weight loss is a pretty big warning sign for colon cancer and Chron’s. If you just have diarrhea and don’t have unexplained weight loss, neither colon cancer or Crohn’s are likely (but they’re still possible).
IBS Diagnosis Table
| If you have | Or if you are | Then you might have |
| Bloating OR constipation OR diarrhea OR bright blood in your stool | Obese OR a smoker OR a user of anti-inflammatories/steroids | Diverticulitis |
| Constipation OR diarrhea OR unexplained weight loss OR fatigue | Over the age of 45 (especially over the age of 65) OR have a history of cancer | Colon cancer |
| Bloody diarrhea | Ulcerative colitis | |
| Diarrhea OR unexplained anemia OR fever OR unexplained weight loss OR growth retardation | Crohn’s disease | |
| Joint pain OR cold intolerance OR constipation OR depression OR heavy menstrual flow OR unexplained weight gain or fatigue OR hair loss | Female | Hypothyroidism |
| Diarrhea AND nausea OR vomiting OR weight loss | In an area with poor water quality or food hygiene standards | Giardia |
| Abdominal bloating OR gas OR distension OR diarrhea | A user of proton pump inhibitors (e.g. Prilosec) OR opioids OR gastric bypass OR colectomy | Small intestinal bacterial overgrowth (SIBO) |
| Diarrhea OR bloating OR fatigue OR anemia OR unexplained blisters (dermatitis herpetiformis) | Type 1 diabetic | Celiac disease |
| Diarrhea | Bile acid malabsorption | |
| Constipation | Over 65 OR African American OR pregnant/a mother | Dyssnergic defecation |
| Abdominal pain and bloating OR gas OR watery stool following the ingestion of foods containing lactose | Black, Latino, or Asian | Lactose intolerance |
| Diarrhea OR constipation OR brain fog OR joint/muscle pain, OR skin rash/dermatitis | Female OR in the third to fourth decade of life | Non celiac gluten sensitivity |
| Nausea and vomiting OR feeling of fullness or burning in your stomach OR blood in your vomit or stool. | In an area with poor water quality or food hygiene standards | H. pylori |
| Constipation OR diarrhea OR nausea OR a feeling of early fullness | A motility disorder, like slow transit constipation | |
| **RARE CONDITIONS FOLLOW BELOW (you probably don’t have these)** | ||
| Constipation since early childhood | Hirschsprung’s disease | |
| Chronic or intermittent watery diarrhea OR unexplained weight loss, OR joint pain | Over 65 OR female | Microscopic colitis |
| Flushing OR diarrhea OR shortness of breath OR palpitation | Carcinoid syndrome (part of carcinoid tumors) | |
| Nausea OR vomiting, OR diarrhea OR anemia OR weight loss | Eosinophilic gastroenteritis |
Steps to treat IBS
If you’ve made it through the whole list above and none of those apply to you, you probably just have IBS.
It’s more likely you have IBS if you have a history of anxiety or depression, are female, or especially if you’ve recently had a stomach bug.
Now you’re looking for treatment. Good on you! My recommendations are to start with a food restriction diet. Take away everything but chicken and rice, then slowly add the rest back in.
If you have diarrhea, you might try a low FODMAP diet, eating small, regular portions, and/or limiting gassy foods like beans, cabbages, and onions.
If you have constipation, you might try psyllium or linseed.
If you want to try medication, I’d recommend very high doses of cholecalciferol (Vitamin D3), like 50k IU every 2 weeks. You might also try peppermint oil for short term diarrhea relief.
That’s my short list. For my long list, including evaluation and limitations of treatments, read on!
IBS Treatment Table
| Potential IBS treatment | Evaluation | Limitations |
| Low FODMAP | Low FODMAP diets seem to work. It doesn’t necessarily work better than just eating normal portions at regular times and reducing fat, insoluble fibers, caffeine, beans, cabbages, and onions. It works better if you have diarrhea. | The studies are only 1-3 months. It’s not clear what happens if you resume a normal diet after that time span. The studies aren’t very well designed. |
| Gluten free diet (for non celiac) | It can work, but there’s not a big effect. | It only works for people who are sensitive to gluten (it’s not for anyone with IBS). |
| Fiber | Bran and insoluble fiber are probably not effective in any form of IBS. Ispaghula (psyllium) and linseed, which are soluble fibers, are probably effective in all forms of IBS. Linseed seems like it’s probably better than psyllium. | All studies were done over a max of 1-3 months. The studies aren’t very well designed. |
| Laxatives | Laxatives work. | They may not prevent constipation, especially in older patients |
| Anti spasmodics (dicyclomine, peppermint oil, pinaverium, trimebutine) | They have ok effects for abdominal pain and bigger effects for overall symptom scores. | |
| Discontinuation of proton pump inhibitors | Not really a cure for IBS, but PPI overuse does lead to SIBO. | |
| Antidepressants | Antidepressants probably work if your IBS is caused by depression or anxiety. It’s unclear whether they work if you don’t. | Antidepressants aren’t more effective in IBS than therapy. It’s unclear if the type of antidepressant matters, but it most likely varies from person to person. |
| Rifaximin | Rifaximin can definitely benefit IBS-D, and may help IBS-C. It doesn’t seem to have any side effects. | |
| Vitamin D3 | Very high doses of vitamin D every 2 weeks (50,000 IU) probably improve IBS symptoms. | Taking really high doses of vitamin D can cause side effects. If you get side effects, stop taking vitamin D. |
| Soy isoflavones | Soy isoflavones may improve IBS in women. | There aren’t really good studies in men. There are no good long term studies either. |
| Acupuncture | Real acupuncture works just as well as fake acupuncture (having someone pretend to stick needles in you). Both work ok. | |
| Probiotics | Probiotics may have a small effect. | The type of bacteria in the probiotic and the formulation matters a lot, as a lot of probiotics are useless or destroyed in the stomach. |
| Mesalazine | Mesalazine is probably not effective in IBS. | |
| Loperamide | Loperamide is helpful for diarrhea and diarrhea-related symptoms. | There aren’t great long-term studies. It may make pain at night worse. |
| Fecal microbiota transplant | Sometimes really helpful, sometimes not helpful at all. | Nasojejunal tube and colonoscopy seem like they work better than capsule for administration. |
Evidence
How I evaluated the evidence
Evaluating evidence is hard in general, and evaluating evidence in IBS is no exception.
I’ll list out those problems, then list how I tried to solve them.
First, there are specific IBS issues.
IBS has a variety of symptoms associated with it, and a treatment that fixes diarrhea will not necessarily fix constipation. This makes treatments difficult to measure in effectiveness. Some scientists try to make up for this by asking patients questions like, “Is your pain reduced?” or “Are you happy with your bowel movements?”, but those can be biased by treatments that treat only pain or depression without affecting IBS-specific symptoms.
To solve this, I tried to tease out the various effects that treatments had on different symptoms of IBS when I could. I paid especially close attention to questions that could be biased, which was a particular issue in antidepressants, as those will obviously make people happier with any treatment.
IBS is also, obviously, really hard to diagnose. One study found that 30% of people with IBS-D actually have bile acid malabsorption. If that’s true, then 30% of the people in any IBS-D study don’t have IBS. What exactly does the study measure, then?
I didn’t have a good way of solving this, so I just hoped for the best.
IBS studies are also often reliant on patient compliance, especially when testing dietary interventions like low FODMAP. This is…not great. This IBD study found only 55% diet compliance (i.e. patients ate different food than prescribed almost half of the time). From my own experience, I had a girlfriend who did weight loss studies. Even when the study gave her food to take home, she would throw it out and just eat her own food because it tasted better. Needless to say, she did not tell the clinicians this.
I tried to solve this by avoiding studies that were reliant on patient compliance and self-reporting. If I couldn’t avoid the studies, I relied on them less for my recommendations.
So, those are some IBS specific issues. Let’s talk about issues in general.
The gold standard for a trial is placebo-controlled, double-blind and randomized. Placebo-controlled means that half the people get a fake treatment, so the experimenters can weed out any people who would have gotten better regardless of if they got the control.
Double blind means that neither the patient nor the experimenters know whether they are getting a real treatment, so nobody can cheat on their measurements or reports if they have a belief one way or another. Last, randomized means people get randomly assigned to placebo or treatment, so we end up with the same sorts of people in both groups.
Reaching that gold standard is easier in some trials than in others. If we’re testing a treatment like gluten, it’s actually surprisingly easy if the experimenters are up for it. They just give every group a pill, and sometimes the pill contains wheat flour, sometimes rice flour. The experimenters don’t know which pills are which until all the measurements are done.
However, if we’re testing a treatment like low FODMAP, it’s impossible. Everyone knows which diet is the low FODMAP diet. There’s no faking it for either side. So, if a patient really believes low FODMAP will work for them, they might be a little more lax with their reports, (if they’re between a 1 and 2 on a scale, they might choose 2 more often than 1). An experimenter might do the same.
I tried to notice when studies were falling away from the gold standard, but I don’t want to just throw away all studies that don’t reach that standard. Then I’d have to throw away a lot of potential useful treatments. Instead, I weighted my judgments accordingly.
Once I was sure studies were performed well, I looked for consistently positive results. Any study can have a positive result once, especially if it’s a small study, in the same way that it’s easy to flip a coin 3 times and get all heads. But consistently getting heads when you flip a coin 100 times is a different story, and suggests there’s actually something there.
I also looked for consistent results across measures. A treatment should improve IBS severity, overall satisfaction, and symptoms. If it only improves one measure, it suggests that measure might have been a fluke.
I also looked for big results in the form of big effect sizes vs. placebo. When there are treatments that can almost quadruple the effects of placebo like vitamin D, small effects like mesalazine which might work ok for some people didn’t cut it.
Last, I combined all these together and got my evaluations.
How I came up with my recommendations
Some technical notes on how to read these.
RR, which is relative risk, is basically the number with the bad outcome over the number with the good outcome. So, the smaller RR is, the better.
CI, which is confidence interval, just accounts for error in the measurement. In the first study below, the RR is estimated to be 0.69, but it might be between 0.54 and 0.88.
I2 (which should really be I2) is a measure of “heterogeneity”, or how different the various effects are. The closer I2 gets to 100%, the greater the differences between studies (which makes you start to wonder why they’re so different).
N, like n=39, is just how many patients there were in a specific group.
The P value, like P=0.62, is the likelihood that a difference found between treatments or conditions is a fluke. By convention, we use P<0.05 to mean significant, as in there’s a less than 5% chance that the difference is a fluke.
[Note for statistics nerds: all the definitions above are rough definitions for a lay audience. If you know the definition better than that, then good on you! Please don’t send me angry messages over it.]
My notes on each study are in italics.
FODMAP
Low FODMAP diets seem to work, but the studies aren’t very good. It doesn’t necessarily work better than just eating regularly and reducing fat, insoluble fibers, caffeine, beans, cabbages, and onions. It works better if you have diarrhea.
All studies were done over 1-3 months.
This is a meta-study for both gluten-free diet and low FODMAP. I used it to guide my thinking, but also looked at the studies myself.
There were seven RCTs comparing a low FODMAP diet with various control interventions in 397 participants. A low FODMAP diet was associated with reduced global symptoms compared with control interventions (RR = 0.69; 95% CI 0.54 to 0.88; I2= 25%). The three RCTS that compared low FODMAP diet with rigorous control diets had the least heterogeneity between studies, but also the least magnitude of effect.
Note that this study is relying on food diaries. This is an ok solution to problems of non compliance, but it’s not great, as people can still lie or misremember. Keeping a food diet for 4 weeks is hard! Also, there’s definitely an overlap between the low FODMAP diet and the normal diet. There’s also no placebo group.
Subjects were randomly assigned to groups that ate specific diets for 4 weeks—a diet low in FODMAPs (n = 38) or a diet frequently recommended for patients with IBS (ie, a regular meal pattern; avoidance of large meals; and reduced intake of fat, insoluble fibers, caffeine, and gas-producing foods, such as beans, cabbage, and onions), with greater emphasis on how and when to eat rather than on what foods to ingest (n = 37).
A total of 67 patients completed the dietary intervention (33 completed the diet low in FODMAPs, 34 completed the traditional IBS diet). The severity of IBS symptoms was reduced in both groups during the intervention (P < .0001 in both groups before vs at the end of the 4-week diet), without a significant difference between the groups (P = .62). At the end of the 4-week diet period, 19 patients (50%) in the low-FODMAP group had reductions in IBS severity scores ≥50 compared with baseline vs 17 patients (46%) in the traditional IBS diet group (P = .72).
This study is looking directly at the metabolome, which is interesting, and should be more reliable than food diaries. The metabolome does seem to change a lot, which is interesting, but it’s weird to look at urine for the metabolome. Urine is not what would normally be affected by a change in diet.
We performed a controlled, single blind study of patients with IBS (Rome III criteria) randomised to a low (n=20) or high (n=20) FODMAP diet for 3 weeks.
Thirty-seven patients (19 low FODMAP; 18 high FODMAP) completed the 3-week diet. The IBS-SSS was reduced in the low FODMAP diet group (p<0.001) but not the high FODMAP group. LBTs showed a minor decrease in H2 production in the low FODMAP compared with the high FODMAP group. Metabolic profiling of urine showed groups of patients with IBS differed significantly after the diet (p<0.01), with three metabolites (histamine, p-hydroxybenzoic acid, azelaic acid) being primarily responsible for discrimination between the two groups. Histamine, a measure of immune activation, was reduced eightfold in the low FODMAP group (p<0.05).
A Diet Low in FODMAPs Reduces Symptoms of Irritable Bowel Syndrome – ScienceDirect
This is a pretty good study. They provided food and they collected stool instead of urine or self-report. Again, there’s no placebo control, so that’s a problem, but this is probably as good as you’re going to get with a low FODMAP diet. I wish they had more people and over a longer term.
In a study of 30 patients with IBS and 8 healthy individuals (controls, matched for demographics and diet), we collected dietary data from subjects for 1 habitual week. Participants then randomly were assigned to groups that received 21 days of either a diet low in FODMAPs or a typical Australian diet, followed by a washout period of at least 21 days, before crossing over to the alternate diet. Daily symptoms were rated using a 0- to 100-mm visual analogue scale. Almost all food was provided during the interventional diet periods, with a goal of less than 0.5 g intake of FODMAPs per meal for the low-FODMAP diet. All stools were collected from days 17–21 and assessed for frequency, weight, water content, and King’s Stool Chart rating.
Subjects with IBS had lower overall gastrointestinal symptom scores (22.8; 95% confidence interval, 16.7–28.8 mm) while on a diet low in FODMAPs, compared with the Australian diet (44.9; 95% confidence interval, 36.6–53.1 mm; P < .001) and the subjects’ habitual diet. Bloating, pain, and passage of wind also were reduced while IBS patients were on the low-FODMAP diet. Symptoms were minimal and unaltered by either diet among controls. Patients of all IBS subtypes had greater satisfaction with stool consistency while on the low-FODMAP diet, but diarrhea-predominant IBS was the only subtype with altered fecal frequency and King’s Stool Chart scores.
Gluten free diet (in non celiac)
Pretty good studies, but there’s not a big effect. All studies were done over 1-3 months.
Again, same meta review.
Both selected patients that had already responded to a GFD, and then randomized them to continue the diet, or to have the diet “spiked” with gluten.
A GFD was associated with reduced global symptoms compared with a control diet (RR = 0.42; 95% CI 0.11 to 1.55; I2= 88%), although this was not statistically significant.
Very skewed women:men ratio. This is “placebo controlled” with normal vs. gluten free muffins. It raises the question of whether the patients could tell the difference between the normal and gluten free muffins, which they probably could.
A total of 34 patients (aged 29-59 years, 4 men) completed the study as per protocol. Overall, 56% had human leukocyte antigen (HLA)-DQ2 and/or HLA-DQ8. Adherence to diet and supplements was very high. Of 19 patients (68%) in the gluten group, 13 reported that symptoms were not adequately controlled compared with 6 of 15 (40%) on placebo (P=0.0001; generalized estimating equation). On a visual analog scale, patients were significantly worse with gluten within 1 week for overall symptoms (P=0.047), pain (P=0.016), bloating (P=0.031), satisfaction with stool consistency (P=0.024), and tiredness (P=0.001).
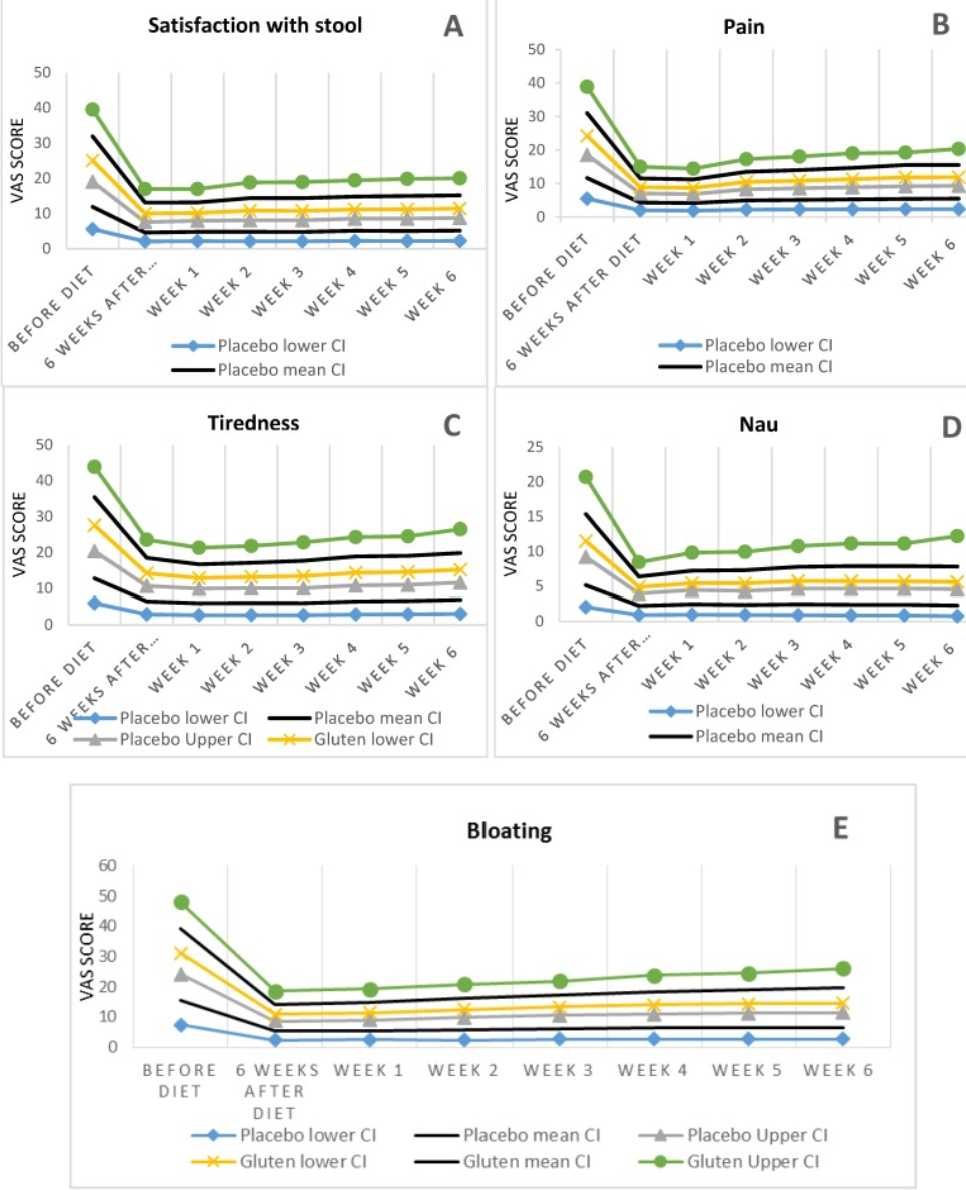
This one is a better placebo because they gave them gluten packets, which would be harder to tell taste wise from gluten free powder. However, the graphs, which I copied below, are terrible and clearly show overlap between placebo and gluten. I’m not a huge fan of this study or how they presented their information, but there does seem to be some effect.
. In the second stage after six weeks, patients whose symptoms improved to an acceptable level were randomly divided into two groups; patients either received packages containing powdered gluten (35 cases) or patients received placebo (gluten free powder) (37 cases). Overall, the symptomatic improvement was statistically different in the gluten-containing group compared with placebo group in 9 (25.7%), and 31 (83.8%) patients respectively (p < 0.001).
Fiber
Bran and insoluble fiber are probably not effective in any form of IBS.
Ispaghula (psyllium) and linseed, which are soluble fibers, are probably effective. Linseed seems like it’s probably better. It’s hard to tell because the studies aren’t very good.
All studies were done over a max of 1-3 months.
This meta analysis has a nice risk ratio graph, which is helpful for us. Note that all the results for bran span both sides of the line, so it’s unclear whether it works.

Laxatives
Laxatives work, but they may not prevent constipation, especially in older patients.
I didn’t feel like I had to really prove this one, to be honest. I got lazy.
Effectiveness of laxatives in adults | BMJ Quality & Safety
Bulk (fibre based) laxatives and osmotic
laxatives (including lactulose and PEG) are
associated with increases in frequency and
improvements in stool consistency and
symptoms of constipation.
+
Little evidence is available at present as to
the comparative effectiveness of bulk and
non-bulk laxatives.
+
There is no good evidence that laxatives
prevent constipation in older patients.
+
A stepped approach to laxative treatment
would seem justified, involving initial inter-
vention with cheaper laxatives, before pro-
ceeding to the more expensive alternatives.
+
There is a pressing need for large compara-
tive trials of diferent strategies for the man-
agement of constipation in adults. This
should include comparisons of the effectiveness of diferent classes of laxative.
+
Research is also required into the effectiveness of overall dietary change (including increased fluid intake) in the treatment of constipation.
Anti spasmodics (dicylomine, peppermint oil, pinaverium, trimebutine)
They have ok effects for abdominal pain and bigger effects for overall symptom scores.
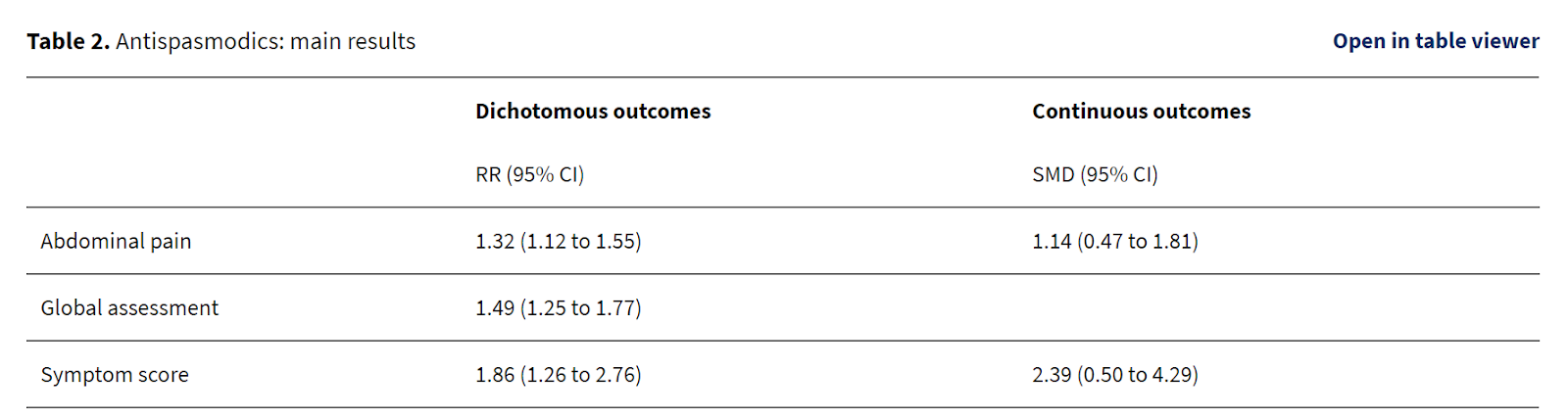
This is a Cochrane review paper. Cochrane is usually seen as the gold standard for reviews, although they’re often too strict.
Also, note that they reverse RR, so RR above 1 is good.
There was a beneficial effect for antispasmodics over placebo for improvement of abdominal pain (58% of antispasmodic patients improved compared to 46% of placebo; 13 studies; 1392 patients; RR 1.32; 95% CI 1.12 to 1.55; P < 0.001; NNT = 7), global assessment (57% of antispasmodic patients improved compared to 39% of placebo; 22 studies; 1983 patients; RR 1.49; 95% CI 1.25 to 1.77; P < 0.0001; NNT = 5) and symptom score (37% of antispasmodic patients improved compared to 22% of placebo; 4 studies; 586 patients; RR 1.86; 95% CI 1.26 to 2.76; P < 0.01; NNT = 3). Subgroup analyses for different types of antispasmodics found statistically significant benefits for cimteropium/ dicyclomine, peppermint oil, pinaverium and trimebutine. Separate analysis of the studies with adequate allocation concealment found a significant benefit for improvement of abdominal pain.
I wanted to look at peppermint oil specifically because that’s what I used to use. It works well according to this study, although note that there’s a rebound between 4 to 8 weeks.
Fifty-seven patients with irritable bowel syndrome according to the Rome II criteria, with normal lactose and lactulose breath tests and negative antibody screening for celiac disease, were treated with peppermint oil (two enteric-coated capsules twice per day or placebo) for 4 weeks in a double blind study. The symptoms were assessed before therapy (T0), after the first 4 weeks of therapy (T4) and 4 weeks after the end of therapy (T8).
At T4, 75% of the patients in the peppermint oil group showed a >50% reduction of basal (T0) total irritable bowel syndrome symptoms score compared with 38% in the placebo group (P < 0.009). With peppermint oil at T4 and at T8 compared with T0 a statistically significant reduction of the total irritable bowel syndrome symptoms score was found (T0: 2.19 ± 0.13, T4: 1.07 ± 0.10*, T8: 1.60 ± 0.10*, *P < 0.01 compared with T0, mean ± S.E.M.), while no change was found with the placebo.
Another study showing an effect of peppermint oil, but I wonder if there was a rebound here, too.
We enrolled 178 consecutive patients affected by IBS, according to the Rome II diagnostic criteria. They were randomized by computer-generated lists to receive either Mintoil 2 capsules t.i.d. before meals for 3 months, or a placebo. A validated questionnaire was administered every 3 weeks to measure the outcome. Data were analysed by χ2 test.
Results. Ninety-one patients (22 M, 69 F; mean age 41 yrs; range 18-72 yrs) received Mintoil, and 87 patients (23 M, 64 F; mean age 44 yrs; range 21-74 yrs) assumed the placebo. Three patients withdrew from the study because of non IBS-related diseases, and two patients because of pyrosis. No other adverse events were recorded.
Peppermint oil, compared to placebo, improved IBS overall symptoms in 73/91 (80%) vs 31/87 (36%) patients (p<0.02). Particularly, significant improvements were achieved for gastroenteric symptoms, in 88/91 (97%) vs 29/87 (33%) patients (p<0.01), psychical discomfort, in 34/91 (37%) vs 16/87 (18%) patients (p<0.05), and socio-familiar impact, in 69/91 (76%) vs 37/87 (43%) patients (p<0.04).
Discontinuation of proton pump inhibitors
This isn’t really an IBS one, but PPIs do lead to SIBO. Discontinuing them may help.
I only really wanted one study for this, because it’s pretty well known, but here you go. They gave patients PPI and accidentally gave them IBS. The other patients who weren’t given PPI didn’t get IBS.
Methods Patients with NERD (acid reflux) not complaining of bowel symptoms were selected by upper endoscopy, 24‐h pH‐metry and a structured questionnaire concerning severity and frequency of bloating, flatulence, abdominal pain, diarrhoea and constipation. Patients were treated with esomeprazole 20 mg bid for 6 months. Prior to and after 8 weeks and 6 months of therapy, patients received the structured questionnaire and underwent evaluation of SIBO by glucose hydrogen breath test (GHBT).
Results Forty‐two patients with NERD were selected out of 554 eligible patients. After 8 weeks of PPI treatment, patients complained of bloating, flatulence, abdominal pain and diarrhoea in 43%, 17%, 7% and 2%, respectively. After 6 months, the incidence of bowel symptoms further increased and GHBT (glucose hydrogen breath test) was found positive in 11/42 (26%) patients. By a post hoc analysis, a significant (P < 0·05) percentage of patients (8/42) met Rome III criteria for irritable bowel syndrome.
Antidepressants
Antidepressants probably make you feel better if you have IBS, in the same way that therapy would. They don’t have any other effects.
Note that well-being improves with paroxetine, which is an antidepressant, but specific IBS related symptoms do not.
In Group 2, overall well-being improved more with paroxetine than with placebo (63.3%vs 26.3%; p = 0.01), but abdominal pain, bloating, and social functioning did not. With paroxetine, food avoidance decreased (p = 0.03) and work functioning was marginally better (p = 0.08). Before unblinding, more paroxetine recipients than placebo recipients wanted to continue their study medication (84%vs 37%; p < 0.001).
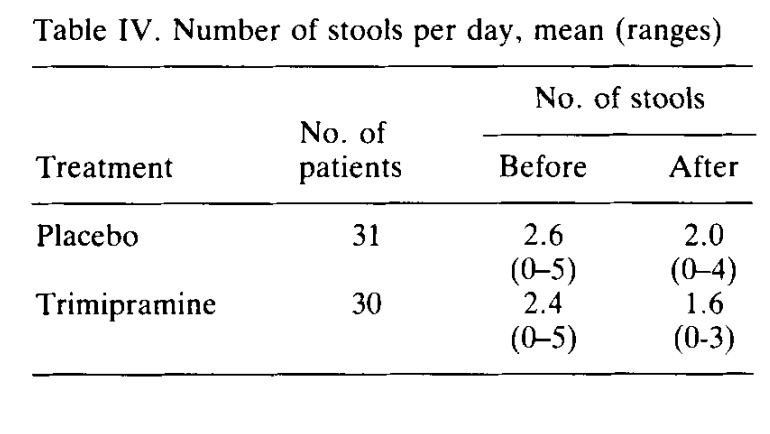
This one shows that trimipramine helps when given a bedtime, for both IBS scores and quality of life. However, I’m not entirely sure what this study is measuring, because there’s a lot of vomiting in this study. IBS patients shouldn’t be vomiting.
61 patients were given either 50 mg trimipramine at bedtime or identically looking coded placebo in a prospective study for 4 weeks. The complaints were graded on an analogue scale by both the patients and the physicians. The results showed that the complaint scores were significantly reduced to about half in the placebo group. In the group treated with trimipramine a significantly greater reduction was found for the scores of vomiting, sleeplessness, depression, and for the mucus content of stools. The scores for tiredness during treatment had decreased less in the group receiving trimipramine than in the one receiving placebo. These improvements occurred already during the first week of treatment.
This is a fun study which compared therapy vs. desipramine, which is an antidepressant. Therapy came out better than desipramine, desipramine came out kind of better than placebo but it’s hard to tell. This one breaks out the “intention to treat” vs. “per protocol”, which basically means that there were a lot of patients who they intended to treat but didn’t (i.e. they dropped out). Also, if you read between the lines, this sort of detailed “subgroup analysis”, where they try to get really specific about who would benefit from desipramine, is usually an attempt to rescue a study that went poorly so they have to find some benefit somewhere. Not a good study!
The intention-to-treat analysis showed CBT as significantly more effective than EDU (P = 0.0001; responder rate, 70% CBT vs. 37% EDU; number needed to treat [NNT ], 3.1). DES did not show significant benefit over PLA in the intention-to-treat analysis (P = 0.16; responder rate, 60% DES vs. 47% PLA; NNT, 8.1) but did show a statistically significant benefit in the per-protocol analysis (P = 0.01; responder rate, 73% DES vs. 49% PLA; NNT, 5.2), especially when participants with nondetectable blood levels of DES were excluded (P = 0.002). Improvement was best gauged by satisfaction with treatment. Subgroup analyses showed that DES was beneficial over PLA for moderate more than severe symptoms, abuse history, no depression, and diarrhea-predominant symptoms;
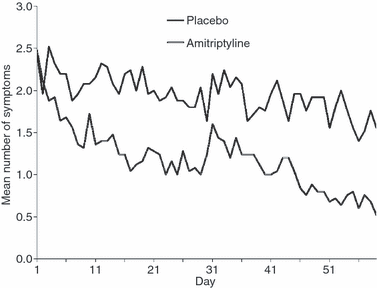
This study seems to have a strong effect for low dose amitriptyline, and was overall a well performed study.
Patients were randomly assigned to receive either 10 mg amitriptyline daily or placebo. Subjects were followed up for 2 months and symptoms were assessed using a questionnaire.
Patients receiving amitriptyline showed greater complete response, defined as loss of all symptoms, compared with those receiving placebo (68% vs. 28%, P = 0.01).
A randomized controlled trial of imipramine in patients with irritable bowel syndrome (nih.gov)
This study has a remarkably high dropout rate, and it’s hard to even know what to think. Why did half the study leave?
One hundred and seven patients were enrolled by advertisement or referral by general practitioners and 56 (31 imipramine: 25 placebo) completed the 16-wk study. Baseline characteristics were comparable. A high overall dropout rate was noted in the imipramine and placebo arms (47.5% vs 47.9%, P > 0.05), a mean of 25.0 and 37.4 d from enrollment, respectively (P < 0.05). At the end of 12 wk, there was a significant difference in global symptom relief with imipramine over placebo (per-protocol: 80.6% vs 48.0%, P = 0.01) and a trend on intent-to-treat (ITT) analysis (42.4% vs 25.0%, P = 0.06). This improvement was evident early and persisted to week 16 (P = 0.024 and 0.053 by per-protocol and ITT analyses, respectively).
This study compared psychotherapy vs. paroxetine vs. routine care. Psychotherapy actually came out on top.
Seventy-two patients with IBS participated in a 12-week, double-blind, randomized, placebo-controlled study of paroxetine-CR (12.5 mg–50 mg/day).
In intent-to-treat analyses, there were no significant differences between paroxetine-CR (N = 36) and placebo (N = 36) on reduction in Composite Pain Scores, although the proportion of responders on CGI–I was significantly higher in the paroxetine-CR group.
Patients with severe IBS were randomly allocated to receive 8 sessions of individual psychotherapy, 20 mg daily of the specific serotonin reuptake inhibitor (SSRI) antidepressant, paroxetine, or routine care by a gastroenterologist and general practitioner.
Both psychotherapy and paroxetine were superior to treatment as usual in improving the physical aspects of health-related quality of life (SF-36 physical component score improvement, 5.2 [SEM, 1.26], 5.8 [SEM, 1.0], and −0.3 [SEM, 1.17]; P < 0.001), but there was no difference in the psychological component. During the follow-up year, psychotherapy but not paroxetine was associated with a significant reduction in health care costs compared with treatment as usual (psychotherapy, $976 [SD, $984]; paroxetine, $1252 [SD, $1616]; and treatment as usual, $1663 [SD, $3177]).
This study weirdly looked at rectal sensitivity as a measure, as well as pain. It showed fluoxetine helped with pain, but not with any IBS specific measures.
Forty non-depressed IBS patients underwent a rectal barostat study to assess the sensitivity to rectal distention before and after 6 weeks of treatment with fluoxetine 20 mg or placebo. Abdominal pain scores, individual gastrointestinal symptoms, global symptom relief, and psychologic symptoms were assessed before and after the intervention
Fluoxetine did not significantly alter the threshold for discomfort/pain relative to placebo, either in hypersensitive (19 ± 3 vs. 22 ± 2 mm Hg above MDP) or in normosensitive (34 ± 2 vs. 39 ± 4 mm Hg above MDP) IBS patients. Overall, 53% of fluoxetine-treated patients and 76% of placebo-treated patients reported significant abdominal pain scores after 6 weeks (not significant). In contrast, in hypersensitive patients only, fluoxetine significantly reduced the number of patients reporting significant abdominal pain. Gastrointestinal symptoms, global symptom relief, and psychologic symptoms were not altered.
This study found an effect of citalopram on pain and bloating, but not really on IBS specific measures.
Twenty three non-depressed IBS patients were recruited from a tertiary care centre and included in a crossover trial comparing six weeks of treatment with the SSRI citalopram (20 mg for three weeks, 40 mg for three weeks) with placebo. IBS symptom severity was the primary outcome measure, and depression and anxiety scores were also measured.
After three and six weeks of treatment, citalopram significantly improved abdominal pain, bloating, impact of symptoms on daily life, and overall well being compared with placebo. There was only a modest effect on stool pattern.
This study found no effect of citalopram.
Patients from primary, secondary, and tertiary care settings were randomly assigned to receive citalopram (20 mg/day for 4 weeks, then 40 mg/day for 4 weeks) or placebo in a study with double-masking and concealed allocation. Symptoms were assessed weekly, and IBS-QOL and rectal sensation by barostat were assessed at the beginning and end of the study.
This study found a big effect of fluoxetine on constipation, and seemed well-performed. They didn’t check if their patients were anxious or depressed, though.
Fluoxetine was significantly more effective than placebo in decreasing abdominal discomfort, relieving feeling and sense of bloating, increasing frequency of bowel movements and decreasing consistency of stool. Mean number of symptoms per patient decreased from 4.6 to 0.7 in the fluoxetine group vs. 4.5 to 2.9 in controls (P < 0.001).
Talley: Antidepressant therapy (imipramine and citalopram… – Google Scholar
This study didn’t find any effect for citalopram, but it did find it for imipramine.
Of 51 IBS patients randomized, baseline characteristics were comparable among the treatment arms; themajority was diarrhea-predominant. Adequate relief of IBS symptoms (primary endpoint) was similar for each treat-ment arm. Improvements in bowel symptom severity rating for interference (P= 0.05) and distress (P= 0.02) were greater with imipramine versus placebo, but improvements in abdominal pain were not. There was a greater improvement in depression score (P = 0.08) and in the SF-36 Mental Component Score (P= 0.07), with imipramine. Citalopram was not superior to placebo. Approximately 20% of the variance in scores was explained by treatment differences for abdominal pain, bowel symptom severity disability, depression and the mental component of the SF-36.
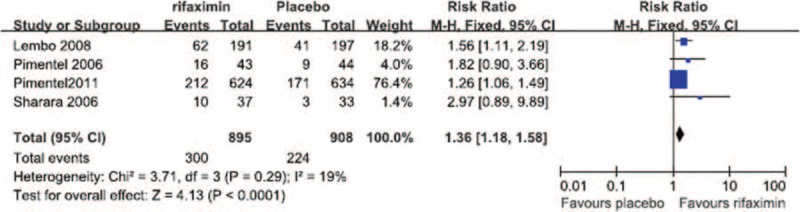
Rifaximin
Rifaximin can definitely benefit IBS-D, and may help IBS-C. It doesn’t seem to have any side effects.
Rifaximin for Irritable Bowel Syndrome (nih.gov)
This is a metastudy of the 4 studies they found that tested rifaximin. Rifaximin came out pretty well.

Abdominal Pain
No significant heterogeneity in the occurrence of abdominal pain during the treatment period was observed between the 3 RCTs in which abdominal pain was reported (I2 = 0%).
Nausea
No significant heterogeneity in the occurrence of nausea during the treatment period was observed between the 3 RCTs in which nausea was reported (I2 = 0%).
Vomiting
No significant heterogeneity in the occurrence of vomiting during the treatment period was observed between the 3 RCTs in which vomiting was reported (I2 = 0%)
Headache
No significant heterogeneity in the occurrence of headache during the treatment period was observed between the 3 RCTs in which headache was reported (I2 = 0%).
Vitamin D
Very high doses of vitamin D every 2 weeks probably improve IBS symptoms.
I like this one because it’s actually long term. It shows remarkably big effects, too.
A total of 90 IBS patients participated in this double‐blind, randomized, placebo‐controlled study. Participants were randomly selected to receive either 50 000 IU vitamin D3 or a placebo fortnightly for a period of 6 months. Patients reported their IBS symptoms at the baseline and monthly during intervention periods
Over the 6‐month intervention period, a significantly greater improvement in IBS symptoms such as abdominal pain and distention, flatulence, rumbling, and overall gastrointestinal (GI) symptoms (except dissatisfaction with bowel habits) was observed in the patients receiving vitamin D as compared to the placebo group. The IBSSS and the IBS‐QoL scores in the vitamin D group significantly improved compared to the placebo group postintervention (mean IBSSS score change: −53.82 ± 23.3 vs −16.85 ± 25.01, p < 0.001, respectively; mean IBS‐QoL score change: 14.26 ± 3 vs 11 ± 2.34, p < 0.001, respectively).
This one also tests isoflavones, and seems to find a bigger effect of soy isoflavones than vitamin D, although both have an effect. It was only for 6 weeks, though. Also, the groups seem really poorly assigned: the before scores are all over the place.
In a factorial blinded randomized clinical trial, 100 women with IBS (age:18-75yr, were randomly assigned in 4 arms to receive either placebo of vitamin D and placebo of soy isoflavones (P+P), or placebo of vitamin D and soy isoflavones (P+S), or vitamin D and placebo of soy isoflavones (D+P), or vitamin D and soy isoflavones (D+S) for 6 weeks. Dosage of soy isoflavone was 2 capsules of 20 mg soy isoflavones per day, and dosage of vitamin D was one pearl of 50’000 IU biweekly. The clinical outcomes were IBS symptoms severity scores (IBS-SSS), disease- specific quality of life (IBS-QOL) and total score (IBS-TS) that evaluated at weeks 0, 6, and 10, and compared to each other.


Soy isoflavones
Soy isoflavones may improve IBS, but it’s hard to tell.
This is just testing soy isoflavones. It’s really hard to tell what’s going on here, as either the soy isoflavones did show some amount of improvement that was almost significant (p value of 0.068), or they actually made things worse.
In a randomized double blind placebo-controlled clinical trial, 67 patients with IBS were allocated to consume either soy isoflavones capsules or a placebo for 6 weeks. The primary outcome was a significant reduction in symptoms severity score and the secondary outcome was a significant improvement in quality of life.
45 participants completed the study. There was no significant changes in mean differences of symptoms severity score between the two groups; however soy isoflavone supplementation could significantly improve the quality of life scores (p=0.009).

Acupuncture
Acupuncture probably doesn’t work better than fake acupuncture.
Acupuncture for treatment of irritable bowel syndrome (nih.gov)
This one seems self-explanatory. Also, I’m biased against acupuncture.
We found no evidence of an improvement with acupuncture relative to sham (placebo) acupuncture for symptom severity (SMD-0.11, 95%CI −0.35 to 0.13; 4 RCTs; 281 patients) or quality of life (SMD = −0.03, 95%CI −0.27 to 0.22; 3 RCTs; 253 patients).
Probiotics
Probiotics may help a little bit but it’s hard to tell. This is compounded by the fact that how probiotics are stored and processed matters a lot to whether they survive all the way to colonize your digestive tract.
Effect of probiotic species on irritable bowel syndrome symptoms:A bring up to date meta-analysis
This study only looked at species, and not at formulation. Also, I don’t trust that some probiotics improve pain, but not distension. That doesn’t make sense.

This is a meta study. It discusses that the only properly performed studies that showed a good effect were on B.infantis.
Sixteen RCTs (n=1,342) met the inclusion criteria. Studies scored between 5 and 12 points on the Rome II methodology scale. Eleven studies were considered to be of suboptimal design (precise definition of suboptimal was not clear).
Two of the appropriately-designed RCTs evaluated Bifidobacterium infantis 35624 and reported statistically significant improvements in abdominal pain/discomfort, bloating/distension and/or bowel movement relative to placebo (p<0.05). In these two trials B. infantis 35624 was given daily for four or eight weeks as 1×1010 live cells in malted milk drink or 1×106, 1×108 or 1×1010 colony forming units per millilitre in capsule form. None of the other studies described as appropriately designed showed significant improvements in IBS symptoms.
No studies reported quantifiable data on relative tolerability or adverse events.
This is a meta study on B. infantis specifically. They found that single B. infantis didn’t help, but combination B. infantis did. That doesn’t really make sense to me. I’d bet it’s a formulation problem.
A total of five studies were identified as suitable for inclusion, including three studies with single probiotic B. infantis and two studies with composite probiotics containing B. infantis. Treatment with single probiotic B. infantis didn’t impact on abdominal pain, bloating/distention, or bowel habit satisfaction among IBS patients. However, patients who received composite probiotics containing B. infantis had significantly reduced abdominal pain (SMD, 0.22; 95% CI, 0.03–0.41) and bloating/distention (SMD, 0.30; 95% CI, 0.04–0.56). After combining the data from six studies, the improvement of bloating/distention among IBS patients remained significant (SMD, 0.21; 95% CI, 0.07–0.35).
Mesalazine
Mesalazine is probably not effective in IBS.
Randomised controlled trial of mesalazine in IBS | Gut (bmj.com)
So, this paper basically found that both placebo and mesalazine had the same “response rate”, which was 67%. Then they tried to rescue it by doing a bunch of complicated statistics, but it really didn’t work that well.
For the primary endpoint, the responder patients were 68.6% in the mesalazine group versus 67.4% in the placebo group (p=0.870; 95% CI −12.8 to 15.1). In explorative analyses, with the 75% rule or >75% rule, the percentage of responders was greater in the mesalazine group with a difference over placebo of 11.6% (p=0.115; 95% CI −2.7% to 26.0%) and 5.9% (p=0.404; 95% CI −7.8% to 19.4%), respectively, although these differences were not significant. For the key secondary endpoint, overall symptoms improved in the mesalazine group and reached a significant difference of 15.1% versus placebo (p=0.032; 95% CI 1.5% to 28.7%) with the >75% rule.
Loperamide
https://link.springer.com/content/pdf/10.1007/BF01296258.pdf#page=1
This study basically showed that loperamide works well.
Loperamide treatment accelerated gastric emptying, compared with placebo (1.2 +- 0.1 vs 1.5 +- 0.1 hr; P < 0.001) and delayed both small bowel (6.2 + 0.3 vs 4.3 + 0.3 hr; P < 0.001) and whole gut transit (56 +- 5 vs 42 +_ 4 hr; P < 0.01). Eighteen patients said they felt better taking loperamide compared with placebo and, at follow up, 15 of these patients remained satisfied with the effects of the drug. Most symptoms improved significantly on placebo compared with the baseline period, but three of these [diarrhea (P < 0.01), urgency (P < 0.01) and borborygmi (P < 0.05)] showed a further significant improvement on loperamide. Improvement in diarrhea was not associated with any change in stool weight but was associated with reductions in stool frequency (P < 0.001), passage of unformed stools (P < 0.01), and incidence of urgency (P < 0.001).
Loperamide improved IBS symptoms, but increased pain at night.
Clinical variables and social and personal relationships were similar for the loperamide group (n = 35), the placebo group (n = 34), the dropouts (n = 21), and the controls. Somatic diseases and mental disturbances were increased in the patients compared with the controls. Throughout the 5 weeks of treatment an improved stool consistency (32%), reduced defecation frequency (36%), and reduced intensity of pain (30%) were found in the loperamide group. An increase in nightly pain was observed in the loperamide group.
Loperamide helped diarrhea but made constipation worse (duh).
In a group of patients with painless diarrhoea (n = 16) there was a highly significant improvement in stool frequency and consistency. In a group with alternating bowel habits and abdominal pain (n = 21) there was also a statistically significant improvement in stool frequency and consistency as well as significantly fewer painful days during loperamide treatment. Patients with alternating bowel habits and no pain (n = 12) experienced no symptomatic improvement, and patients with constipation (n = 9) generally felt worse on loperamide. No side effects were encountered.
Loperamide helps diarrhea and diarrhea-related symptoms.
The effects of loperamide in patients with IBS (all had diarrhoea as a main symptom) were studied in a double-blind placebo controlled trial. Subjective overall response, stool consistency and six individual symptoms (urgency, pain, frequency, flatulence, borborygmi and painful propulsions) were studied over a 13 week long treatment period. Twenty-one patients out of 25 completed the trial, 11 in the loperamide group and 10 in the placebo group. A significant advantage for loperamide was found for stool consistency (p<0.001), pain (p<0.02) and urgency (p<0.05). Subjective overall response was also significantly better in the loperamide group (p<0.03).
Fecal transplant
Results vary really widely. Worth a shot if you’re desperate.
This meta analysis threw out half the studies for not being well-performed. The rest are presented below. Note that two of them show a big positive effect, and two of them do not. The two negative ones did capsule, the two positive ones did colonoscopy and nasojejunal tubes.

How I came up with my list of diagnoses
Diverticulitis
Symptoms & Causes of Diverticular Disease | NIDDK (nih.gov)
Most people with diverticulosis do not have symptoms. If your diverticulosis causes symptoms, they may include
- bloating
- constipation or diarrhea
- cramping or pain in your lower abdomen
In most cases, when you have diverticular bleeding, you will suddenly have a large amount of red or maroon-colored blood in your stool.
Studies have found links between diverticular disease—diverticulosis that causes symptoms or problems such as diverticular bleeding or diverticulitis—and the following factors:
- certain medicines—including nonsteroidal anti-inflammatory drugs NIH external link (NSAIDs), such as aspirin NIH external link, and steroids NIH external link
- lack of exercise
- obesity
- smoking
Testing for colon cancer:
About 70% of patients with colon cancer are >65 years of age and the disease is rare under the age of 45 (2 per 100 000/year).
Colorectal cancer most commonly occurs sporadically and is inherited in only 5%–10% of cases. Migrant studies indicate that when populations move from a low-risk area (e.g. Japan) to a high-risk area (e.g. the USA), the incidence increases rapidly within the first generation of migrants.
Smoking has consistently been associated with large colorectal adenomas, which are generally accepted as precursors for cancer. An updated review suggested a temporal pattern consistent with an induction period of three to four decades between genotoxic exposure and the diagnosis of colorectal cancer. In the USA one in five colorectal cancers may be potentially attributable to tobacco use.
Inflammatory bowel diseases (Crohn’s disease and ulcerative colitis) increase the risk of colon cancer
Patients who have had previous malignant disease are also at great risk of developing a second colorectal tumour
The metabolic syndrome (high blood pressure, increased waist circumference, hypertriglyceridaemia, low levels of high-density lipoprotein cholesterol or diabetes/ hyperglycaemia) had a modest, positive association with colorectal cancer incidence among men, but not among women
Because early cancer produces no symptoms and because many of the symptoms are non-specific (change in bowel habits, general abdominal discomfort, weight loss with no apparent cause, constant tiredness),
Up to now two strategies have been available: faecal occult blood test (FOBT) and endoscopy.
Influence of dietary factors on colorectal cancer survival (nih.gov)
Colorectal cancer (CRC) is one of the most common cancers in the Western world. It is widely accepted that environmental factors, especially dietary factors, are involved in the aetiology of CRC. High intakes of fat, red meat, refined sugar, and energy have been associated with an increased risk of CRC
Inflammatory bowel disease
The Diagnostic Approach to Monogenic Very Early Onset Inflammatory Bowel Disease – ScienceDirect
Twin studies have provided the best evidence for a genetic predisposition to IBD, which is stronger for CD than UC.
Genetic disorders that affect intestinal epithelial barrier function include dystrophic epidermolysis bullosa,32 Kindler syndrome,32 familial diarrhea caused by dominant activating mutations in guanylate cyclase C,33 X-linked ectodermal dysplasia and immunodeficiency,34 and ADAM17 deficiency.35
As high as 40% of patients with chronic granulomatous disease develop CD-like intestinal inflammation.
VEOIBD has been described in a number of hyperinflammatory and autoinflammatory disorders such as mevalonate kinase deficiency,54, 55 phospholipase C-γ2 defects,56 familial Mediterranean fever,57, 58, 59 Hermansky–Pudlak syndrome (type 1, 4, and 6),60, 61, 62, 63, 64 X-linked lymphoproliferative syndrome type 165 and type 2,66, 67, 68 or familial hemophagocytic lymphohistiocytosis type 5
Disorders associated with IBD-like immunopathology include B-cell defects such as common variable immunodeficiency (CVID), hyper-immunoglobulin (Ig) M syndrome, and agammaglobulinemia.75, 76, 77, 78, 79 Several other primary immune deficiencies, such as Wiskott–Aldrich syndrome80 (WAS) and atypical SCID or Omenn syndrome81, 82 can also cause IBD-like intestinal inflammation.
Cow’s milk protein allergy is common and can cause severe colitis that resembles UC and even requires hospitalization. It manifests typically within the first 2 to 3 months of exposure to cow’s milk protein. This may be apparent with breast-feeding or only after introducing formula feeding. Colitis resolves after cow’s milk is removed from the diet, so a trial of exclusive feeding with an amino acid–based infant formula is a customary treatment strategy for all VEOIBD diagnosed when the patient is younger than 1 year of age.
Bloody diarrhea is the most common presenting symptom in UC whereas CD may present with vague abdominal pain, diarrhea, unexplained anemia, fever, weight loss, or growth retardation as frequently reported symptoms. The classic “triad” of abdominal pain, diarrhea, and weight loss occurs in only 25% of patients with CD
Hypothyroidism
Hypothyroidism: an update: South African Family Practice: Vol 54, No 5 (tandfonline.com)
Arthralgias (joint pain)
Cold intolerance*
Constipation
Depression
Difficulty concentrating
Menorrhagia (heavy flow)
Myalgias (muscle pain)
Weakness
Weight gain
Dry skin
Fatigue*
Hair thinning/hair loss
Memory impairment
Hyperthyroidism
Hyperthyroidism affects 3% of women and 0.3% of males (1) and is associated with significant morbidity and mortality, mainly from cardiovascular and cerebrovascular disease (2, 3). In iodine-replete areas, the underlying diagnosis is Graves’ disease in 60–80% and toxic nodular hyperthyroidism in most others (4, 5). Patients commonly complain of fatigue, anxiety, tremor, weight loss, palpitation, and heat sensitivity. Clinical signs include tachycardia, the presence of goiter, and a tremor
Giardiasis
Transmission of Giardia is via the faecal–oral route, either indirectly through contaminated water or food, or directly from person to person.
Giardia infection is usually associated with diarrhoea, but can be either asymptomatic or responsible for a broad clinical spectrum, with symptoms ranging from acute to chronic [4]; diarrhoea can occur with or without malabsorption syndrome; there can be nausea, vomiting, and weight loss [5]. Occasionally, Giardia infection can be associated with pruritis and urticaria [6], uveitis [7], sensitisation towards food antigens [8,9] and synovitis [10]. Children might also suffer more serious consequences, including retarded growth and development [11,12], poor cognitive function
Carcinoid syndrome
CSy is defined as symptoms and signs of overproduction of serotonin produced by neuroendocrine tumor, such as flushing, diarrhea, dyspnea, bronchospasm, palpitation, and eventually, symptoms associated with right-sided heart failure resulting from carcinoid heart [Bhattacharyya et al. 2007].
Microscopic colitis
Sci-Hub | Diagnosis and Management of Microscopic Colitis | 10.1038/ajg.2016.477 (scihubtw.tw)
The most common symptom in patients with microscopic colitis (MC) is chronic or intermittent watery diarrhea, ranging in severity from mild to severe with dehydration and electrolyte abnormalities. Other symptoms are commonly present, including abdominal pain, weight loss, and arthralgias, each present in up to half of patients
However, the presence or absence of certain clinical features, such as older age, female sex, use of certain medications or recent initiation of any medication, weight loss, nocturnal stools, and shorter duration of diarrhea, may identify patients at higher or lower risk of having MC
Small intestinal bacterial overgrowth
Small Intestinal Bacterial Overgrowth: Clinical Features and Therapeutic Management (nih.gov)
Although abdominal bloating, gas, distension, and diarrhea are common symptoms, they do not predict positive diagnosis. Predisposing factors include proton-pump inhibitors, opioids, gastric bypass, colectomy, and dysmotility.
Eosinophilic gastroenteritis
Eosinophilic gastroenteritis: diagnosis and clinical perspectives (nih.gov)
Mucosal EGE is the most common variety, seen in about 57%7 to 100%8,9 of cases, and presents with features of abdominal pain, nausea, vomiting, dyspepsia, diarrhea, malabsorption, or protein-losing enteropathy, which in turn may cause hypoalbuminemia, anemia, and weight loss. Additionally, the occurrence of lower-GI bleeding may imply colonic involvement.
Celiac disease
Celiac disease: From pathophysiology to treatment (nih.gov)
Dermatitis herpetiformis is an inflammatory cutaneous disease, presenting with diffuse, symmetrical, polymorphic lesions consisting of erythema, urticarial plaques, papules, herpetiform vesiculae and blisters followed by erosions, excoriations and hyperpigmentation. It is characterized by typical histopathological and immunopathological findings. Rarely it is diagnosed in childhood but commonly appears in the third decade.
Type 1-diabetes
One of the most recognized and widely investigated disorders associated with celiac disease is type 1-diabetes
Autoimmune thyroid disorders
In patients affected by celiac disease it has been reported an increased prevalence (nearly, 2%-5%) of thyroid disorders (i.e., hyperthyroidism-Graves’s disease or hypothyroidism-Hashimoto’s thyroiditis), diagnosed either before than after the diagnosis of gluten-enteropathy
Autoimmune hepatitis and other forms of liver involvement
The involvement of liver is common among patients affected by celiac disease
Life-long gluten-free diet
The current available treatment for celiac disease is life-long gluten-free diet[91–93]. Generally clinical improvement is achieved within a few weeks and the mucosal damage recovers in 1-2 years
Bile acid malabsorption
Altered concentrations of bile acid (BA) in the colon can cause diarrhea or constipation. More than 25% of patients with irritable bowel syndrome with diarrhea or chronic diarrhea in Western countries have BA malabsorption (BAM)
Although BAM is recognized in practice, the most popular current method of diagnosis includes a therapeutic trial of BA binders with symptom improvement; this approach is prevalent and the only resource available in countries like the United States where the noninvasive imaging based on scintigraphic BA retention is unavailable. Unfortunately, in certain disease states, symptoms may only improve with high doses of a BA sequestrant or binder, and the diagnosis of BAM may be missed
Dyssnergic defecation
Diagnosis and Treatment of Dyssynergic Defecation (nih.gov)
Constipation is more common in women with an estimated female:male ratio of 2.2:1.10 Its prevalence increases with advancing age, particularly after age 65.10 African Americans,10 lower socioeconomic status,10 pregnancy,14 and neurological diseases including Parkinson’s disease and multiple sclerosis.
The etiology of dyssynergic defecation is unclear. In a prospective survey of 118 patients with dyssynergia, we found that the problem began during childhood in 31% of patients, and after a particular event, such as pregnancy, trauma, or back injury in 29% of patients, and there was no cause in 40% of patients
Lactose intolerance
Lactose Intolerance – American Family Physician (aafp.org)
Common symptoms include abdominal pain and bloating, excessive flatus, and watery stool following the ingestion of foods containing lactose. Lactase deficiency is present in up to 15 percent of persons of northern European descent, up to 80 percent of blacks and Latinos, and up to 100 percent of American Indians and Asians
Non celiac gluten sensitivity
Recent advances in understanding non-celiac gluten sensitivity (nih.gov)
In addition to experiencing GI symptoms, patients with NCGS most often experience a complex of extra-intestinal symptoms, including a “foggy mind”, which is described as an inability to concentrate, reduction of mnemonic capabilities, and lack of well-being as well as tiredness, headache, anxiety, numbness, joint/muscle pain, and skin rash/dermatitis
According to self-reported data, the prevalence rate of NCGS ranges between 0.5% and 13% in the general population 2– 5, and prevalence is higher in women 2, 3, teenagers, and patients in the third to fourth decade of life 2, 4.
Helicobacter pylori
A review of Helicobacter pylori diagnosis, treatment, and methods to detect eradication (nih.gov)
H. pylori infection affects nearly half of the world’s population. In developing countries, the prevalence of infection is as high as 90%, whereas in developed countries, excluding Japan, the prevalence is below 40%
Today, the involvement of H. pylori in active chronic gastritis, its association with gastroduodenal ulcer, and its well-accepted role as a risk factor for the development of gastric cancer are well documented[68].
Gastritis | Cedars-Sinai (cedars-sinai.org)
Stomach upset or pain
Belching and hiccups
Belly (abdominal) bleeding
Nausea and vomiting
Feeling of fullness or burning in your stomach
Loss of appetite
Blood in your vomit or stool. This is a sign that your stomach lining may be bleeding.
Helpful info from Wikipedia that I didn’t feel like checking
Causes
- Neurological/psychiatric: A study of 97,593 individuals with IBS identified comorbidities such as headache, fibromyalgia, and depression.[79] IBS occurs in 51% of people with chronic fatigue syndrome and 49% of people with fibromyalgia, and psychiatric disorders occur in 94% of people with IBS.[10]
- Channelopathy and muscular dystrophy: IBS and functional GI diseases are comorbidities of genetic channelopathies that cause cardiac conduction defects and neuromuscular dysfunction, and result also in alterations in GI motility, secretion, and sensation.[80] Similarly, IBS and FBD are highly prevalent in myotonic muscle dystrophies. Digestive symptoms may be the first sign of dystrophic disease and may precede the musculo-skeletal features by up to 10 years
Epidemiology
| Canada | 6%[150] | Boivin, 2001 | |
| Japan | 10%[151] | Quigley, 2006 | Study measured prevalence of GI abdominal pain/cramping |
| United Kingdom | 8.2%[152]10.5%[153] | Ehlin, 2003Wilson, 2004 | Prevalence increased substantially 1970–2004 |
| United States | 14.1%[154] | Hungin, 2005 | Most undiagnosed |
| United States | 15%[150] | Boivin, 2001 | Estimate |
| Pakistan | 14%[155] | Jafri, 2007 | Much more common in 16–30 age range. 56% male, 44% female |
| Pakistan | 34%[156] | Jafri, 2005 | College students |
| Mexico City | 35%[157] | Schmulson, 2006 | n=324. Also measured functional diarrhea and functional vomiting. High rates attributed to “stress of living in a populated city.” |
| Brazil | 43%[151] | Quigley, 2006 | Study measured prevalence of GI abdominal pain/cramping |
| Mexico | 46%[151] | Quigley, 2006 | Study measured prevalence of GI abdominal pain/cramping |
Gender
Women are around two to three times more likely to be diagnosed with IBS and four to five times more likely to seek specialty care for it than men.[158
Studies of females with IBS show symptom severity often fluctuates with the menstrual cycle, suggesting hormonal differences may play a role.[159]